
Risk, awareness, and aftercare — RACK and SSC in practice, reading a body’s real signals, keeping impact safe, and aftercare that actually lands.
Foundations
Safety 101
Not optional infrastructure — the structure that lets everything else we do exist. Reading the body, knowing the danger zones cold, and trusting the instinct to step back from a scene that’s wrong.
Safety isn’t optional infrastructure for BDSM — it’s the structure that lets the rest of what we do exist. This lesson goes deeper than the framework names: reading the body in real time, the danger zones to know cold, sub-drop and top-drop, first-aid awareness, substances, the health conditions that change the calculus, and the instinct to step back from a scene that’s wrong even when nothing specific is broken. It builds on the Consent module.
Consent is the “yes.” Safety is making sure the yes can be honoured. The two are inseparable: consent from a partner who doesn’t understand the risks isn’t real consent, and a scene without basic safety practices isn’t honouring the consent that was given.
What you’ll be able to do
By the end of this lesson, you’ll be able to…
- Read a partner’s body in real time — breath, limb colour, tension, face — and distinguish deep subspace from genuine distress.
- Recognise the signs that mean stop-and-assess now, and recall the impact map of never-zones versus safe targets.
- Anticipate sub-drop and top-drop, and plan aftercare across all three timescales.
- Assemble a basic safety kit and apply first-aid awareness to the foreseeable emergencies — knowing where the line to call for help sits.
- Evaluate how substances and health conditions change what’s safe, and trust the instinct to step back from a scene that’s wrong.
Here is the shape of the lesson. We start where Consent left off — re-reading the frameworks you already know through a safety lens — then move outward through the body itself: learning to read it in real time, telling a deep state apart from distress, and knowing the signals that mean stop. From there the lesson maps the territory of harm and recovery: where impact lands safely and where it never can, the drop that follows an intense scene, and the aftercare that catches it. Then the practical core — first-aid awareness, the kit, and the way substances and health conditions change what is safe tonight. We close on the judgment that ties it together: the positions that mute a partner, the bottom who pushes past their own limits, and the instinct to step back from a scene that is simply wrong.
In this lesson: the frameworks and reading the body (§ I–III) · stopping signs and the impact map (§ IV–V) · drop and aftercare (§ VI–VII) · first aid, the kit, substances and health (§ VIII–IX) · judgment: muted partners, the press-in pattern, and the step-back instinct (§ X–XII).
I.The Frameworks, From a Safety Angle
You met SSC / RACK / PRICK in Consent. Re-read through the safety lens.
SSC — a good floor
For lower-risk play between long-term partners, it’s the whole conversation. Its limit (“safe” implies risk can be eliminated) only matters when you’re doing things where it genuinely can’t.
RACK — the honest default
Most of what people do at OTT carries residual risk no skill removes. RACK requires you understand it specifically — not “this might leave a mark” but “this can cause nerve damage in this spot.”
PRICK — who does the homework
You don’t get to consent to risks you don’t understand. A bottom consenting to rope without knowing about nerve compression isn’t informed — and neither is the top. Read the risks, watch competent practitioners, ask until your map is sharp.
II.Reading the Body
Negotiation gave you the map; the scene shows you the territory. Most of safety is reading what your partner shows you, in real time, and adjusting.
Breath
The most informative signal. Faster during impact is normal. Sudden changes are information: a gasp that doesn’t resolve, a held breath too long, ragged breathing that doesn’t match the rhythm.
Limb temp & colour
The bondage-specific signal. Cold or pale = circulation compromised; bluish or purple = already significant. Touch the extremities — don’t just watch them.
Tension
Information, not an alarm — some play produces it. Watch for sudden shifts: relaxed to rigid against the activity, or going completely limp when you’d expect engagement.
Face & skin
Eyes drifted far away or a face gone suddenly flat deserve a check-in. Sudden sweating (or sweat stopping), and goose-pimples without cold or arousal, can signal a stress or panic response.
None of these is a single-symptom alarm — they’re inputs to your reading of the whole. The mistake is fixing on one (“breathing is steady”) and treating it as the entire picture.
III.Distress vs Deep State
A bottom who’s stopped responding to check-ins could be in deep subspace, dissociation, or acute distress — and from outside they look nearly identical.
The honest move is to pause and assess, not stop completely. Pausing isn’t ending. Shift to attentive presence — a hand on the shoulder, a quiet voice — and see how they respond. Some come up enough to say “keep going,” some to say “I need to come out,” some don’t come up easily and you stay in pause until they do.
Don’t continue because breathing is steady — breathing alone is not enough information; you don’t know what they’re inside until you check. And introduce no new activity from this state: as you learned in Consent, new consent cannot be given from subspace.
IV.Stopping Signs
Some signals mean stop the scene immediately to assess — regardless of where you were in the plan. Others don’t, on their own.
Stop & assess now
- Loss of verbal response when it was expected.
- Limb temperature or colour change — cold, pale, blueish (circulation).
- Unexpected bleeding from somewhere you’re not working.
- Sudden breathing change unrelated to the activity — gasping, can’t slow it.
- Loss of motor control that doesn’t match the activity; limbs going limp.
- Cold sweat in someone previously warm; bleeding from mouth or nose without cause.
Not a stop on its own
- Sweating and faster breathing during impact — normal physiology.
- A grunt or a curse — people make noise; read context.
- Tension that matches the activity.
- Pain — the point of some activities. The question isn’t “is there pain?” but “is it still landing the way negotiation said it would?”
Pick a scene you actually want to try, then run a risk check on it: name the two or three “stop & assess now” signs most likely to show up in that activity, and decide in advance what your first move is when you see each one. Knowing them cold beforehand is what lets you act in the half-second you have.
V.Impact Zones
The basic map for paddles, floggers, canes, crops. Know it cold — four zones, not two, and some of the “avoid” damage is internal and invisible.
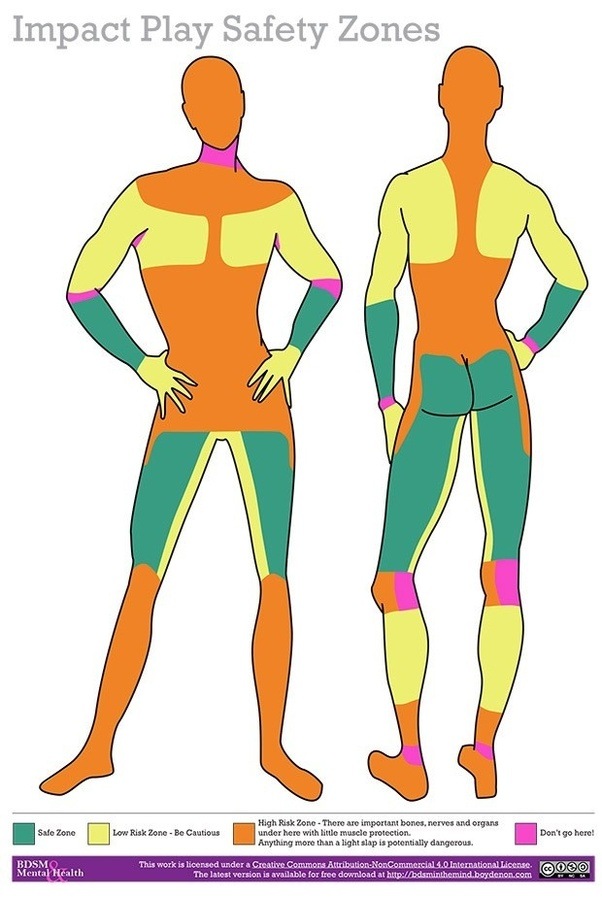
Safe Zone
- Buttocks — the standard target.
- Front of the thighs — muscular and forgiving (the inner-thigh stripe is low-risk, not safe).
- Backs of the thighs — lots of muscle.
- Forearms — well-tolerated for lighter impact.
Low-Risk Zone — be cautious
- Shoulders & upper chest — tolerable, but thinner than they look.
- Upper back / shoulder blades — keep off the spine itself.
- Calves — only the well-muscled belly; the bone and back of the knee are not.
- Wrists and the inner-thigh stripe — ease off the pressure here.
High-Risk Zone
- Head & face — eyes, nose, teeth, plus the bruise-visibility issue.
- Mid & lower torso, belly — liver, spleen, gut sit right under thin muscle.
- Kidneys (lower back / flank) — can rupture; damage is internal.
- Hips, groin, hands, knees, shins, feet — important bones, nerves and organs under here with little muscle protection; anything more than a light slap is potentially dangerous.
- Nape (back of the neck) and the full back over the spine — nervous system runs through it.
Don’t go here!
- Front of the throat — the trachea.
- Elbows — bony, poorly cushioned, nerve-exposed.
- Backs of the knees — nerves and vessels sit right at the surface.
- Ankles — bone and tendon, no protection.
Within the safe and low-risk zones there’s still variation. A cane on the back of the thigh near the knee can cause nerve damage if it lands wrong; a heavy thuddy flogger across the upper back is fine where a sharp implement isn’t. The zone tells you the ceiling; the tool and the strike decide whether you stay under it.
VI.Sub-Drop & Top-Drop
The emotional/physical crash that can follow an intense scene — endorphin and adrenaline depletion. It happens to bottoms and tops.
Subdrop usually shows up hours to days after: emotional fragility, sudden weepiness, irritability, anxiety, fatigue beyond the exertion, mild depression, “what does this mean about me.” Even a scene that went perfectly can produce significant drop. Top-drop hits similarly and is less discussed — guilt, replay-loops, a flat emptiness the day after a scene that was great in the moment. Tops feel less entitled to ask for aftercare, which makes top-drop both more common and more isolating.
What helps
- Knowing it’s coming — an expected drop lands softer.
- Connection — text, call, or sit with someone in the dynamic.
- Basic self-care: food, water, sleep, gentle movement, sunlight.
- Routine, and talking the scene through when you’re both ready.
What makes it worse
- Isolation — drop alone tends to spiral.
- Straight from an intense scene to high-stakes work or obligations.
- Alcohol or other substances to “manage” it.
- Treating drop as evidence something was wrong with the scene. It usually isn’t.
If drop is severe, lasts more than a few days, or comes with thoughts of self-harm — reach beyond your immediate partner: a BDSM-aware therapist, a trusted senior member, or a mental-health professional.
VII.Aftercare Timescales
Three timescales — skipping any of them is how aftercare becomes performative.
Immediate (mins–hrs)
Warmth, water, food, sitting close. Letting the bottom come back at their own pace — and the top too. End the scene with enough time and energy reserved for this.
Next day or two
The drop check-in. “How are you doing today?” — that’s the whole conversation. Especially important after intense play or with someone you don’t know well.
Longer (days–weeks)
Reflection in a calm context — what worked, what didn’t, what to adjust. How one scene becomes better future scenes.
Chronic conditions reshape this: a bottom with arthritis may flare two days after significant kneeling; a partner with anxiety may need a longer reflection conversation. Disability, age, and pre-existing pain all change aftercare needs — the negotiation should cover it.
VIII.First-Aid Awareness & Emergency Planning
You don’t need to be a medic. You do need to know what to do for the foreseeable things, and where the line is past which you call someone who is.
| Situation | What to do |
|---|---|
| Bleeding | Firm pressure with clean material — most stops in five minutes. If it won’t slow, or blood is spurting (arterial), call emergency services. |
| Loss of consciousness | Don’t revive aggressively. Clear airway, position on their side, call emergency services if they don’t come round within seconds. |
| Bondage emergency | Have safety (paramedic) shears accessible to the rope/cuff. Cut, don’t untie, if there’s urgency. Train this before you need it. |
| Burns | Cool with running water 10–15 min. Don’t pop blisters. Severe or large-area burns get medical attention. |
| Fracture / dislocation | Immobilise; don’t try to “put it back.” Get medical care. |
| Allergic reaction | If breathing is affected, call emergency services. Mild material reactions (latex, lubricant): remove it, clean the area. |
Have on hand, even in a private space
At OTT events, DMs are trained for the safety role and carry additional supplies. Get to know your DM before you need them, and know where the kit, the exit, and the help are.
Build your own safety kit from the checklist above and put it where you actually play — not in a drawer across the house. Then walk one first-aid scenario out loud: where are your shears, could you reach them one-handed, and at what point would you stop and call for help? Locate the gap now, while it costs nothing.
IX.Substances & Health
Two big inputs to what’s safe right now.
Significant alcohol impairs judgment, slows reactions, suppresses pain perception (so you miss harm), and dehydrates. Cannabis alters time and pain perception — don’t introduce it mid-scene if you haven’t established what it does to your scene state. Stimulants spike heart rate and blunt your sense of your own limits. Painkillers mute the pain signal you’d otherwise use to track injury. Multiple substances magnify all of it. Negotiation happens sober; play needs the alertness of operating equipment.
Some health conditions change what’s safe, what aftercare looks like, or how recovery works. Disclose them; if you’re the partner, treat the disclosure as input, not a deal-breaker. None of these is a permanent ban on BDSM — they’re inputs the negotiation should explicitly accommodate.
| Condition | What it changes |
|---|---|
| Cardiovascular (high BP, arrhythmia, cardiac history) | Intense scenes spike heart rate; restraint can drop blood pressure. Reshapes which activities are appropriate. |
| Respiratory (asthma, COPD) | Rules out positions/activities that further restrict breathing. |
| Joint & spinal (bad knees, discs, replacements) | Restraint positions and impact targets need adjustment. |
| Diabetes | Blood sugar can drop in intense scenes. Keep glucose on hand; the drop check-in matters more. |
| Bleeding disorders / anticoagulants | Bruising and bleeding are harder to predict or stop. |
| Mental health (anxiety, depression, PTSD, bipolar) | Don’t require avoiding BDSM, but shape which scenes are healthy and what aftercare needs to be. Negotiate explicitly. |
| Pregnancy / recent surgery | Change everything — many activities become inappropriate until recovery. Negotiate from scratch. |
X.Positions That Limit Communication
Some activities reduce your partner’s ability to signal. Plan for it — verbal check-ins become more important, not less.
Gags
Remove speech entirely. Negotiate a non-verbal safeword — three rapid taps, dropping a held object. Don’t gag a new partner before you’ve practised the alternative.
Suspension
Off the ground, often unable to move enough to signal. Demands a competent rigger who knows nerve points, circulation, and emergency descent. Learn it in person from someone qualified, not from a book.
Sensory deprivation
Blindfolds, hoods, headphones remove input. Combined with restraint it’s high-trust territory — have a clear plan for how the bottom signals when you’re not in direct contact.
Chest / diaphragm pressure
Positions that press the chest can interfere with breathing without the bottom being able to say so. Have them breathe deeply in the position before you commit to time in it.
XI.The “Press-In” Pattern
Some bottoms push past their own limits — for performance, or because they’ve learned not to ask for what they need. Dangerous, because their self-report is the very thing you rely on to keep them safe, and they’re over-riding it.
Signs: insisting they’re fine when their body says otherwise, escalating beyond what was negotiated, refusing the safeword they agreed to, treating hitting a limit as a failure to push through.
Pause, check in, set a stricter intensity ceiling than the bottom is asking for — and hold it even when they push back. This is one of the rare cases where the top’s judgment legitimately over-rides the bottom’s in-scene preference: not to override consent, but to protect the consent process from being eaten by a performance reflex. If you are that bottom, name it to your partner up front and ask them to set a ceiling and hold it — that request is itself an act of consent.
XII.Trust the Step-Back Instinct
Mid-scene, something feels wrong — not a specific stopping sign, just an instinct that it shouldn’t continue. Trust it. Pause, investigate, decide.
The cost of pausing a fine scene is small — a few minutes of disrupted flow, easily recovered. The cost of not pausing a scene that should have been paused is large and sometimes irreversible. The asymmetry runs in favour of pausing. Almost every bad scene has the “I knew it was wrong but I kept going” thought attached afterward — train yourself to trust the instinct in the moment, before it becomes a retrospective regret. This goes for both roles.
“It was going so well we just kept playing” is a common story in scenes that ended badly. Going past the negotiated window needs a deliberate decision to extend, not inertia — long scenes use more energy, accumulate more low-grade injury, and shrink the aftercare runway. The signal isn’t how the scene feels; it’s how much you’re asking your bodies to absorb.
Next event you attend, before you play: find the nearest exit and locate the DM on duty — put a name to them, even just a hello. Knowing where the exit and the help are before the moment you need them is the difference between acting on the step-back instinct and freezing on it.
If you remember one thing: safety is the structure that lets the yes be honoured — and most of it is reading your partner in real time and being willing to pause. When one signal says “fine” but something else says “wrong,” the asymmetry always favours stopping: the cost of pausing a good scene is minutes, the cost of not pausing a bad one can be irreversible. Everything else here — the body-reading, the maps, the kit, the conditions — serves that one instinct.